
 |  |  |
|
|
|
|||||||
|---|---|---|---|---|---|---|---|---|
|
|
|
Sunday, January 10, 2010



























Monday, January 4, 2010
Medical/Surgical Nursing
Medical/Surgical Nursing
Johns Hopkins Bayview Medical Center’s medical and surgical nursing units are staffed by dedicated professionals committed to quality care, patient education and customer satisfaction. Our medical and surgical nurses provide a continuum of care in a variety of settings, including adult medicine, surgical units, orthopaedics, neuroscience, telemetry and the Johns Hopkins Burn Center.
Medical/surgical nursing units at Johns Hopkins Bayview include:
Our medical/surgical nursing graduates participate in 12 weeks of unit-specific, individualized orientation for medical or surgical areas (MedA, MedB, GSurg, A4W, Neuroscience, Progressive Care and Burn Unit). Experienced RNs receive individualized, preceptored orientation for six to eight weeks. Six-month operating room internships are also available, featuring classroom instruction and skill development. Medical and surgical nurses also have the opportunity to participate in many internal and external continuing education programs.
Johns Hopkins Bayview Medical Center’s medical and surgical nursing units are staffed by dedicated professionals committed to quality care, patient education and customer satisfaction. Our medical and surgical nurses provide a continuum of care in a variety of settings, including adult medicine, surgical units, orthopaedics, neuroscience, telemetry and the Johns Hopkins Burn Center.
Medical/surgical nursing units at Johns Hopkins Bayview include:
- Surgical Unit
- Orthopaedic Unit
- Burn/Wound Unit
- Progressive Care Unit
- Neurological Care Unit
- Med A Unit
- Med B Unit
Our medical/surgical nursing graduates participate in 12 weeks of unit-specific, individualized orientation for medical or surgical areas (MedA, MedB, GSurg, A4W, Neuroscience, Progressive Care and Burn Unit). Experienced RNs receive individualized, preceptored orientation for six to eight weeks. Six-month operating room internships are also available, featuring classroom instruction and skill development. Medical and surgical nurses also have the opportunity to participate in many internal and external continuing education programs.


Integrated Medical and Surgical Gastroenterology
$94.97
van Lanschot
2006
718 pp, 210 illustrations
hardcover
ISBN (Americas): 9781588904232
ISBN (EUR, Asia, Africa, AUS): 9783131424211
This Textbook covers the entire spectrum of both benign and malignant gastrointestinal disorders. It is unique in its multidisciplinary approach and focuses on practical issues in day-to-day clinical care.
The complexity of novel diagnostic modalities and the great variety in therapeutic options, both medically and surgically, require an integrated, multidisciplinary approach. Therefore, each topic in this Textbook is first discussed by two gastroenterologists and subsequently by two digestive surgeons. If appropriate, interventional radiologists, internists and pathologists have also contributed. Specific subchapters on gastrointestinal malignancies have been added, written by medical and radiation oncologists.
Nowadays, many hospitals and medical schools change their infrastructure from discipline-oriented to patient-/disease-oriented. In fact, this Textbook describes what the medical gastroenterologist should know about surgical gastroenterology and vice-versa. A large number of drawings in full color helps the reader to get a clear picture of many technical procedures.
2006
718 pp, 210 illustrations
hardcover
ISBN (Americas): 9781588904232
ISBN (EUR, Asia, Africa, AUS): 9783131424211
This Textbook covers the entire spectrum of both benign and malignant gastrointestinal disorders. It is unique in its multidisciplinary approach and focuses on practical issues in day-to-day clinical care.
The complexity of novel diagnostic modalities and the great variety in therapeutic options, both medically and surgically, require an integrated, multidisciplinary approach. Therefore, each topic in this Textbook is first discussed by two gastroenterologists and subsequently by two digestive surgeons. If appropriate, interventional radiologists, internists and pathologists have also contributed. Specific subchapters on gastrointestinal malignancies have been added, written by medical and radiation oncologists.
Nowadays, many hospitals and medical schools change their infrastructure from discipline-oriented to patient-/disease-oriented. In fact, this Textbook describes what the medical gastroenterologist should know about surgical gastroenterology and vice-versa. A large number of drawings in full color helps the reader to get a clear picture of many technical procedures.
Medical & Surgical Intervention
No matter what type of liver disease you have, we offer treatment options. The approach will depend on a number of factors, such as what type of liver disease you have, your general health, your age and gender, and how far your disease has progressed at the time it is diagnosed.
For liver cancer treatment, we may recommend a medical solution, such as intra-arterial chemoinfusion (chemotherapy), radiofrequency ablation (using radio waves to destroy cancer cells) or cryoablation (using extreme cold to destroy cancer cells). Alternatively, we may suggest a surgical option for treatment, including liver transplantation.
For liver cancer treatment, we may recommend a medical solution, such as intra-arterial chemoinfusion (chemotherapy), radiofrequency ablation (using radio waves to destroy cancer cells) or cryoablation (using extreme cold to destroy cancer cells). Alternatively, we may suggest a surgical option for treatment, including liver transplantation.
Specialized Ultrasound Solutions
Specialized Ultrasound Solutions
The market leader in urological and surgical ultrasound machinesOur BK Medical subsidiary, located in Denmark, is the market leader in specialized ultrasound systems used primarily in urology and surgery. For the past 30 years, BK Medical has been devoted to the development and production of high-quality diagnostic ultrasound systems.The Flex Focus™ is the newest member of BK’s scanner family. A full-size scanner with superior image quality in a small, mobile system, the Flex Focus is revolutionizing the portable ultrasound machine market. Using IQPACTM technology with enhanced tissue definition, image quality is dramatically improved. For information on the Flex Focus and other BK Medical ultrasound products, please visit www.bkmed.com. | ||
Sound Technology A global leader in the design, development, and manufacture of diagnostic medical ultrasound transducersOur Sound Technology subsidiary, located in State College, Pennsylvania, provides customized ultrasound probes to medical OEMs and clinicians. Founded in 1987, Sound Technology has consistently provided customers with superior probe technology for a wide range of ultrasound applications including radiology, cardiology, obstetrics and gynecology, and surgery.STI’s portofolio of probes includes:
|


Saturday, January 2, 2010
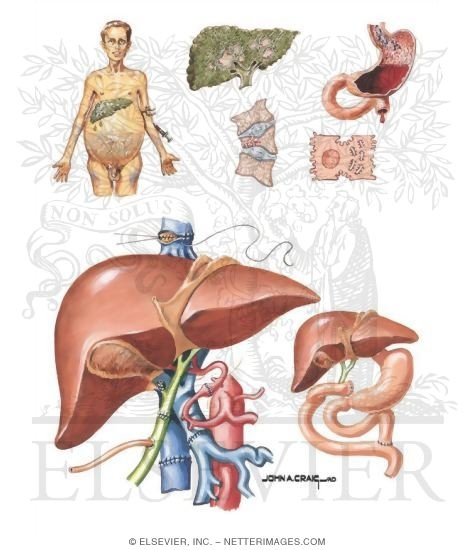
Other Versions of This Illustration
This Illustration was Published In
Netter's Gastroenterology
Author: Martin H. Floch, MD, Neil R. Floch and Kris V. Kowdley
Chapter: Liver Transplantation
Page: 800
Author: Martin H. Floch, MD, Neil R. Floch and Kris V. Kowdley
Chapter: Liver Transplantation
Page: 800
McGilvray Veterinary Hospital
Surgery Suite
The surgery suite is where all sterile surgical procedures, such as spays and neuters, take place. We perform a wide array of soft tissue and orthopedic surgeries, as well as laparoscopic and endoscopic procedures. All of our surgical patients receive intravenous fluids as well as conscientious anesthetic monitoring by one of our Registered Veterinary Technicians.

Services
Veterinary Emergency & Referral Group is open 24/7 to accept emergency and critical patients. The primary veterinarian is requested to alert VERG that an emergency case is being sent to our hospital from their office if possible. Should your hospital or clinic be closed during certain hours or on certain holidays, VERG will accept your pets if your primary veterinarian is unavailable. Patients referred for emergency treatment or care will be referred back to their primary veterinarian for continued care, upon the completion of treatment at VERG. Specialty Services By Appointment:
Please arrive early to fill out an information sheet. Be sure to bring the following with you:
Please arrive early to fill out an information sheet. Be sure to bring the following with you:
- Pertinent medical and surgical history information
- List of symptoms/signs of illness
- List of any medications the animal takes
- X-rays or other lab results, if needed
- Referral forms when applicable
- Payment
- Neurology

- No referral or appointment needed for Emergency Care
- 24 Hour/365 Day Emergency Service
- Veterinarian and trained technicians always in attendance
- Critical Care monitoring
- Emergency surgical procedures
- Emergency endoscopies
- Oxygen cages
- Heated recovery cages
- ECG
- Blood Pressure monitoring
- Isolation
- Digital x-rays
- Endoscope
- Full in house Laboratory
- Ultrasound

- Orthopedic surgery
- Thoracic surgery
- Abdominal surgery
- Reconstructive surgery
- Head and neck surgery
- Imaging Procedures (abdominal or thoracic ultrasound)
- Video Endoscopy (including: gastroduodenoscopy, broncoscopy, proctoscopy, colonoscopy)
- Endocrine Testing (including: adrenal, thyroid, parathyroid, insulin and sex hormone evaluations)
- Bone Marrow Biopsies and aspirates
- Tumor Biopsies
- Transtracheal Washes
- Blood Pressures
- Diagnosis and management of autoimmune disorders

- Diagnostic and therapeutic procedures
- Cataract removal
- Laser surgery for glaucoma
- Electroretinograms
- Electrocardiography
- Echocardiography
- Doppler Studies
- Contrast Ecocardiography
- Holter Monitoring
- Cardiac Event recording
- Cardiac Catheterization
- Epilepsy
- Vestibular Disease
- Meningitis / Encephalitis
- Neuropathy / Myopathy
- Myasthenia Gravis
- CNS Neoplasia
- Intervertebral Disc Disease
- Congenital brain/spinal disorders
- MRI / CSF analysis

- Comprehensive Consultations
- Allergy Testing
- In house Preparation of Allergy Vaccines
- Skin Biopsies - Dermatohistopathology
- Bacterial and Fungal Cultures
- Cytology
- Skin Scrapings
- Laboratory Tests
- Radiation Therapy
- Chemotherapy
- Surgical Oncology

- radiology consultation and diagnostic
- ultrasound imaging services
- CT
- MR neuro- and musculoskeletal- imaging
- radioiodine therapy program for hyperthyroid cats
- Spinal Disease
- Intracranial Disease
- Epilepsy
No Appointment or Referral is needed for Emergency Services
Open 24/7, 365
718-522-9400
Open 24/7, 365
718-522-9400
Payment
We will provide a good-faith low-end and high-end range estimate for cost of our services before treating your pet. In most situations, a full deposit of the low-end estimate is required before treating your pet. Payment in full is needed upon discharge of your pet. We accept cash, Visa, MasterCard, Discover and CareCredit ®. CareCredit ® is a flexible payment program, specifically designed for healthcare expenses that makes it easier for you to get the treatment or procedures that your pet needs. If you plan to use CareCredit ® to finance your bill, you may apply at our front desk, or online.
GIST Support International - Surgical Procedures for Primary GIST

These are only general descriptions. The surgeon's approach in an actual case depends on factors such as:


If removal of the upper rectum is required, the divided end of the colon may be connected to the remaining rectum at the time of tumor removal. Another option may include removal of the rectum and creation of a colostomy with the plan to return later to reconnect the bowel to remaining rectum or the anus, usually forming a pouch of colon tissue to serve as a substitute reservoir for improved bowel continence.
If the GIST is close to or involves the anal sphincter muscles, then an operation called abdominoperineal resection of the rectum (APR) may be performed. This involves removal of the anus and rectum. The end of the remaining sigmoid colon is brought out through the surface of the abdomen in a permanent colostomy.

Surgical Procedures for Primary GIST
This page describes the more common types of surgeries to remove primary gastrointestinal stromal tumors (GISTs). GIST Support International gratefully acknowledges the kind expert review of this material by surgical oncologist Christopher Windham, MD FACS. Dr. Windham heads the Florida Hospital Cancer Care Institute in Daytona Beach. You can read Dr. Windham's tutorial Abdominal Anatomy for GIST in our website's Ask the Professional section.These are only general descriptions. The surgeon's approach in an actual case depends on factors such as:
- the exact anatomical site of the GIST
- characteristics of the individual patient's particular situation
- specific location of the GIST relative to the blood supply of the involved organ
- whether or not the GIST has adhered to, surrounded, or invaded adjacent structures
- the patient's overall medical condition.
The Gastrointestinal Tract.. [Figure from National Cancer Institute]
In most cases the GIST grows outward from the wall of the GI tract into the abdomen rather than growing into the interior of the digestive organs. This is in contrast to the common GI cancers (carcinomas) that grow inside the digestive tract from its lining tissues.Esophageal Surgery for GIST
GISTs occur in the esophagus only rarely (perhaps 2% of GISTs). Other tumor types are more common in the esophagus. The esophagus presents a difficult surgical challenge due to its location beneath the breastbone (sternum), posterior to the heart and between the lungs. Sometimes a local excision or tumor enucleation may be used for a very small esophageal GIST. However, for larger tumors most of the esophagus is removed in an esophagectomy. The following diagram illustrates how the stomach is brought up through the space formerly occupied by the esophagus.Normal esophagus (left) and esophagectomy. [Figure from National Cancer Institute]
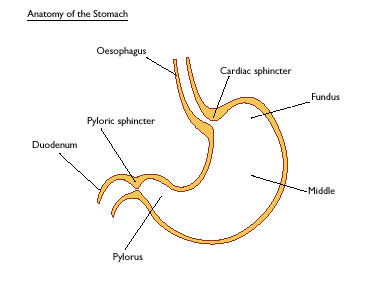
Gastric Surgeries for GIST
- The cardiac sphincter between the esophagus and the stomach: If this must be removed then the patient will have reflux from the stomach into the esophagus, especially if lying down too soon after eating a meal.
- The pyloric sphincter between the stomach and the duodenum: If this must be removed then the stomach will empty quickly after eating, reducing both digestion and absorption of food in the stomach and potentially causing dumping syndrome, also called early gastric emptying.
Lower esophagus (labeled oesophagus per British spelling) and the parts of the stomach. [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk ]
Wedge partial resection of the stomach
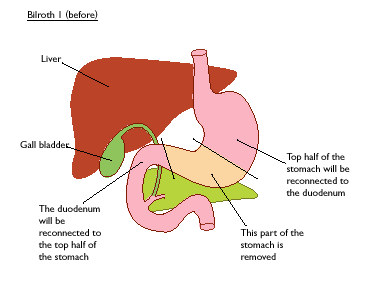
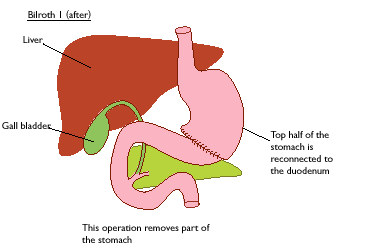
This may be done as an open surgery (laparotomy) or as a laparoscopic surgery. A wedge of stomach tissue containing the origin of the GIST is removed together with the tumor. The cut edges of the stomach where the wedge was removed are brought together and re-joined. If the surgeon uses a stapler, the section of stomach to be removed (including the tumor) is pinched up, and the stapler is used to cut it out and re-join the edges in one step. Because only a portion of the stomach is removed, wedge resection does not require complex reconstructionBillroth I partial gastrectomy, or gastroduodenostomy
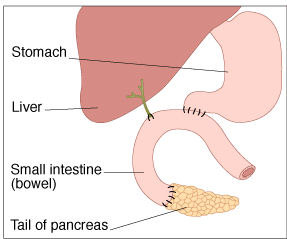
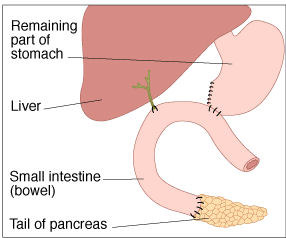
Billroth I Surgery: Before (top panel) and after (bottom panel). [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk ]
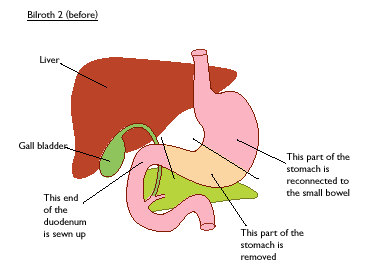
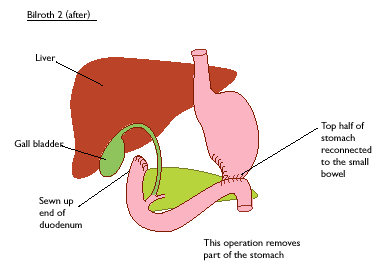
Billroth II partial gastrectomy, or gastrojejunostomy
In this surgery a variable portion of the lower stomach is removed, and the cut border is attached to the jejunum (small bowel) past the duodenum. The duodenum is retained to preserve the bile duct and pancreatic duct, but the bile and pancreatic enzymes do not meet the food to be digested until they flow from the duodenum into the jejunum.Billroth II Surgery: Before (top panel) and after (bottom panel). [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk]
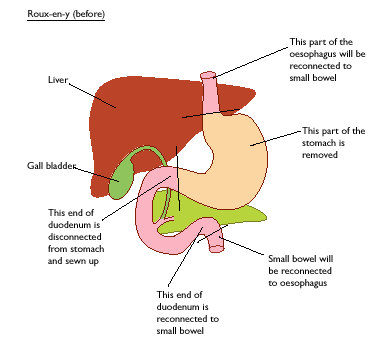
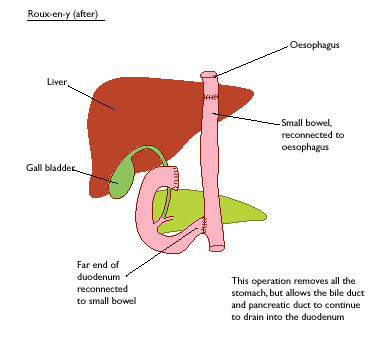
Total gastrectomy with Roux-en-Y reconstruction
If the tumor involves the upper stomach or the gastro-esophageal junction then a total gastrectomy may be needed. In this case the esophagus is attached to the jejunum, as shown in the next figure. The disconnected duodenum is retained to keep the ducts through which bile and pancreatic enzymes enter the GI tract.Roux-en-Y Total Gastrectomy: Before (top panel) and after (bottom panel). [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk]
Duodenal Surgeries for GIST
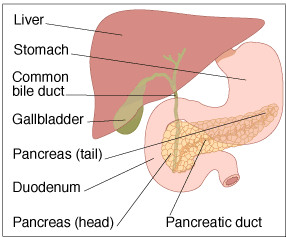
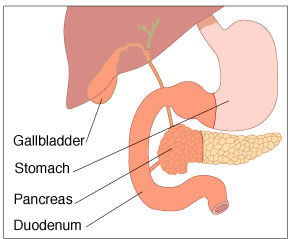
The duodenum is the first section of the small intestine; it is about 9 inches long, shaped in a distinct C curve around the head of the pancreas. It accepts partially digested food from the stomach through the pyloric sphincter. Additional digestive juices are secreted by the walls of the duodenum, further assisting digestion. Bile produced by the liver (to help digest fats) enters the duodenum through the bile duct from the gall bladder, which is an outpouching of the bile duct that acts as a reservoir for bile. Pancreatic digestive enzymes enter the duodenum through the pancreatic duct. The bile duct and pancreatic duct join together and enter the duodenum at a common point called the ampulla of Vater. The C-shape of the duodenum and the ducts emptying into it are shown in the next figure.Anatomic relationship of the duodenum and surrounding structures. [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk]
Partial Resection of Duodenum
Only about 5% of GISTs arise from the duodenum. If a GIST is small and is attached to a section of the duodenum far enough away from the ampulla of Vater, then it may be possible to perform a segmental resection of just the portion of the duodenum to which the tumor is attached.Pancreaduodenectomy (Whipple resection)
For duodenal GISTs that involve the bile ducts or are very close to the ampulla of Vater, and for GISTs that are adherent to adjacent organs, a complex operation known as a "Whipple resection" or pancreaduodenectomy is needed. In this surgery the duodenum is removed along with the gall bladder, common bile duct, distal stomach, and the head of the pancreas. In some cases the surgeon can leave the entire stomach and pyloric sphincter intact (pylorus sparing pancreatoduodenectomy).Pre-surgery anatomy (top panel) and pancreaduodenectomy either sparing the pylorus (second panel) or with resection of the pylorus (third panel). [Figure graciously provided by CancerHelp UK, the patient information website of Cancer Research UK, www.cancerhelp.org.uk]
Segmental resection of the jejunum, ileum, or colon for GIST
The small bowel (small intestine) and large bowel (colon) are where many nutrients are absorbed from digested food. The anatomical names duodenum, jejunum, and ileum describe the three successive sections of the single continuous tube that is the small intestine. Duodenal GIST was discussed previously. GISTs arising from the colon are rare (about 2%), but about 20% of GISTs do originate from the jejunum or ileum. The small and large bowels are essentially hollow tubes. Therefore, a segment where a GIST is growing may be removed and the cut ends reattached. Think of a leaky garden hose, and how you could cut out the bad section and then splice the remaining parts back together.Surgery for rectal or anal GIST
Only about 5% of GISTs develop from the rectum and anus. The rectum serves as a reservoir for solid waste matter. This material is expelled when the anal sphincter relaxes to permit a bowel movement. A partial resection of the rectum may be used if a rectal tumor is not too close to the anal sphincter muscles. In this situation a temporary colostomy or ileostomy may be constructed to allow healing and minimize the significance of a leak (should one occur). A colostomy refers to the creation of a new exit for solid waste matter by routing the colon to exit the body through a surgically created opening (stoma) through the abdominal wall. A collection bag is attached to the stoma.If removal of the upper rectum is required, the divided end of the colon may be connected to the remaining rectum at the time of tumor removal. Another option may include removal of the rectum and creation of a colostomy with the plan to return later to reconnect the bowel to remaining rectum or the anus, usually forming a pouch of colon tissue to serve as a substitute reservoir for improved bowel continence.
If the GIST is close to or involves the anal sphincter muscles, then an operation called abdominoperineal resection of the rectum (APR) may be performed. This involves removal of the anus and rectum. The end of the remaining sigmoid colon is brought out through the surface of the abdomen in a permanent colostomy.
Subscribe to:
Posts (Atom)